- Start
- FA-INFO-KIT
- Infopool
Ansprechpartner & Unterstützung
Die DFA-Hilfe an Ihrer Seite
- Oral Screening
- Kontakt
Add-on Screening
Prevention of Oral Cancer
Oral Screening in patients with Fanconi anemia
using brush-biopsy

Special Characteristics of Fanconi Anemia
Young High-Risk Patients
Patients with Fanconi anemia (FA) have a significantly increased risk of developing squamous cell carcinoma. These highly aggressive tumors occur at an unusually early age in this population and without the patients being exposed to typical toxins such as alcohol and tobacco.
Restricted Therapy
Due to the underlying DNA repair defect in FA, these patients are also hypersensitive to many classic chemotherapeutic agents. Therefore, standard protocols for treating oral carcinomas cannot be applied to patients with FA.
Oral Screening
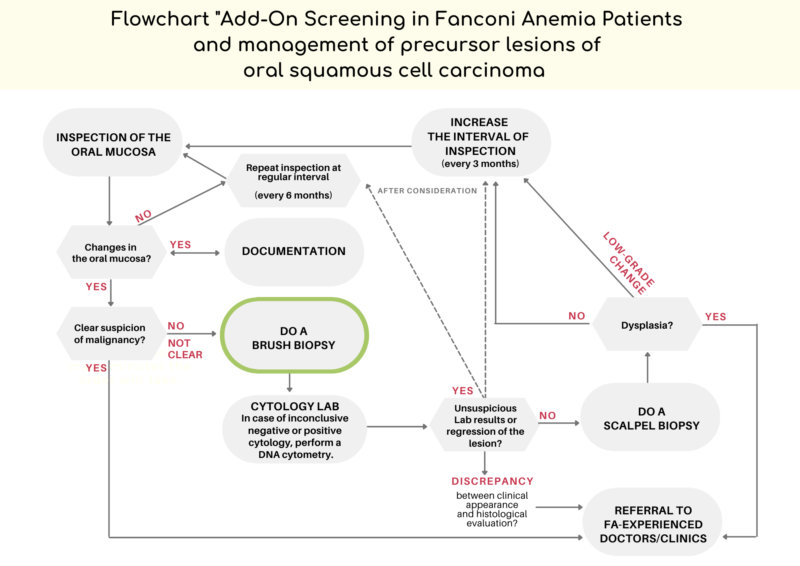
Screening for the early detection of oral tumors and their precursor lesions is therefore particularly important for these patients.
A challenge in clinical practice is that FA patients often have visible changes in the oral mucosa, so not every lesion can be clarified through invasive biopsy.
Despite the increased risk of oral cancer in FA patients, most visible changes are (still) not precancerous.
Brush-biopsy as a Tool for Screening
A large prospective study demonstrated the diagnostic reliability of non-invasive brush biopsies for assessing visible oral lesions through cytological analysis in the FA population.
Based on the findings of the study, the „Add-on Screening for Oral Cancer Prevention in Patients with Fanconi Anemia“ was developed.
Screening vs Diagnosis
The goal of the Add-on Screening is to utilize brush biopsy as an additional tool in the screening process (vs. as a tool for diagnosis of cancer).
When used in this manner, changes in visible lesions of the oral mucosa can be cytologically determined very early in the course. The progression of a lesion to severe dysplasia can thus be more intensively monitored, allowing for early initiation of steps towards histological diagnosis or therapy.
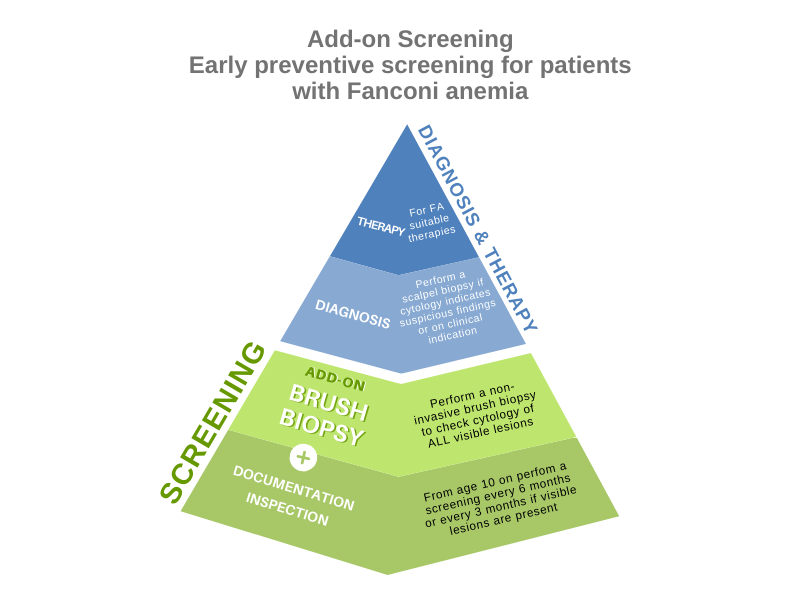
Basics of Add-on Screening
Study / Download
The study titled
demonstrated the diagnostic reliability of non-invasive brush biopsies for assessing visible oral lesions through cytological analysis in the FA population.
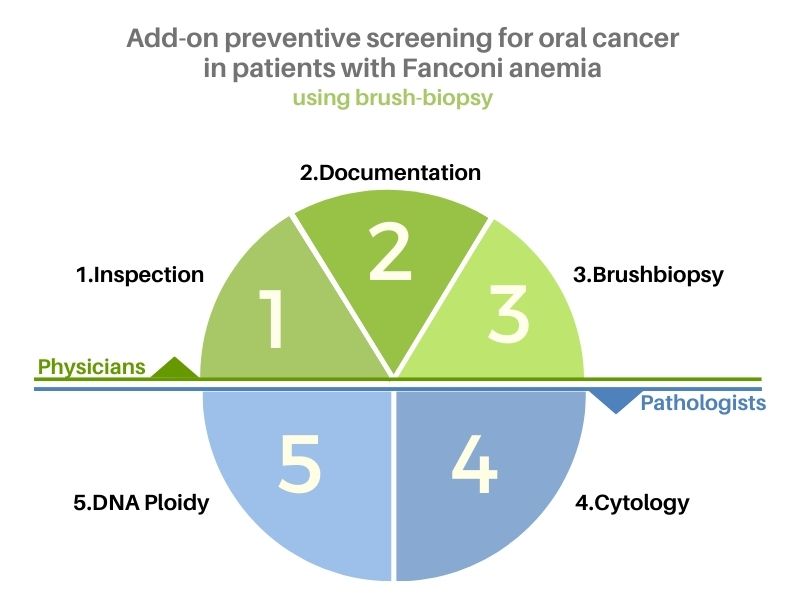
Step-by-Step Instructions / SOP Download
Here you can download a PDF containing all the fundamentals of the study. It includes descriptions of all the steps of the Add-on Screening process (inspection, documentation, brush biopsy, and laboratory/cytological analysis).
Download here all SOPs (Standard Operating Procedures) for Add-on Screening.
Regular Screeningprogram for adults with FA
HERE is an overview of the preventive examinations that adults with FA should undergo regularly.
Materials & Instructions
Process of Oral Inspection
Frequently, potentially malignant oral lesions in patients with FA are small and thus easily overlooked. Therefore, the inspection of the oral cavity should be conducted systematically to ensure no area is missed, for example:
- Inspection of the outer gingiva starting from the upper right quadrant, continuing with the remaining quadrants including the retromolar region.
- Inspection of the inner parts of the gingiva following the same pattern.
- Inspection of the palate, palatal arches, and tonsils.
- Inspection of the tongue: dorsal surface, lateral borders, ventral surface.
- Inspection of the floor of the mouth.
- Inspection of the right and left cheeks including the buccal sulci.
- Inspection of the lips.
Visible changes in the oral mucosa in patients with FA are common. Squamous cell carcinomas in patients with FA often occur in the visible parts of the oral cavity. The tongue and the gingiva of the posterior teeth are particularly affected.
Process of Documentation
The photo documentation of every visible lesion is essential to better assess changes over time such as size, surface texture, consistency, color, etc., especially for lesions that often persist.
Moreover, precise anatomical documentation is necessary. The use of a mouth map in addition to clear text description has proven to be very reliable. Precise anatomical documentation enables:
- Performing an invasive biopsy at the exact same location if there is an abnormal cytological result.
- Better matching of photos and swabs in case of multiple lesions.
The mouth map should remain in the patient’s file with the swabbing physician.
Both documentation systems also contribute to increased transparency and comparability when exchanging information with medical colleagues and the patient.HERE you can download a graphical mouth map (PDF) for documenting found lesions.
Download Oral map
HERE you can download a graphical mouth map (PDF) for documenting found lesions.
Brush biopsy materials
We recommend the following materials for performing a brush biopsy:
Cell collectors:
Orcellex brushes (Rovers Medical Devices, Oss, The Netherlands)
Transport containers with fixation medium:
BD SurePath (BD Biosciences, Heidelberg, Germany)
Process of taking Brush biopsy
Procedure of Brush Biopsy
In this hands-on video, you can learn how to perform a brush biopsy.
Rotate the cell collectors (brushes) with good pressure 15 times on the visible oral lesion, either clockwise or counterclockwise. It’s important to maintain the same direction of rotation to avoid losing already collected cells by changing the direction.
Transfer the brush into the transport container with fixation medium.
If necessary (e.g., if the visible mucosal change is in a difficult anatomical location or if you feel you haven’t collected enough cells with one brush), use a second brush and repeat the process, then transfer the second brush into the same transport container as the first one.
Rotate the two brushes against each other. If you’ve only used one brush, rotate it against the inner wall of the container.
Detach the brushes from the holder (Orcellex model) by pushing down the transparent part of the holder and close the container. For brush models with a fixed brush head, the protruding stem can be cut with scissors.
Gently shake the container with the brush heads to release the cells into the fixation medium.
The samples can be shipped at room temperature via regular mail without time pressure.
Reference lab for FA-samples
The German Cytopathology Laboratory of the University of Düsseldorf is very experienced in analyzing samples from FA patients. We recomend to get in touch with Dr. Schramm.
Contact:
Dr. M. Schramm Martin.Schramm@med.uni-duesseldorf.de Telefon: +49-211-8119346
Address:
departement of Cytopathologie, Universitätsklinikum Düsseldorf, Building 14.81, Moorenstr. 5,
40225 Düsseldorf
Intro-Video Oral prevention in FA
Hands-on Video: Instruction on brush biopsy




Years observed (2006-2018)
0
FA-Patients around the world
0
Brush Biopsies of FA-Patients
0
Sensitivity through Brush Biopsy (Cytology & DNA Ploidy)
0
%
Specificity through Brush Biopsy (Cytology & DNA Ploidy)
0
%
Negative predictive value
0
%